
This opinion piece by Health Fund President David Jordan originally appeared in the Kansas Reflector on November 10, 2022, the first in a two-part series on current and emerging challenges and how Kansans are looking ahead to develop innovative solutions and ensure health care for generations to come. View part 2: Looking ahead, here’s how we can support the health care workforce of a changing Kansas
To plan for the future and better understand the health care workforce crisis, United Methodist Health Ministry Fund commissioned research examining the current health professional education pipeline in Kansas.
Health care is vital for our communities, but our ability to maintain the workforce needed to adequately deliver that care is under pressure. In this two-part series, we look at current and emerging challenges, as well as how Kansans are looking ahead to develop innovative solutions and ensure health care for generations to come.
Kansas faces many challenges in delivering health care, especially in rural areas. The state is experiencing shifting demographics, uninsurance rates higher than the national average, and difficulty attracting and retaining workers.
As we plan for the future, we need to consider how outside factors will affect demand for workers, who we are recruiting to the health care workforce, where and how they will be trained, how technology will impact care delivery, and where providers will need to be located.
Kansas’ population trends will affect demand and workforce composition
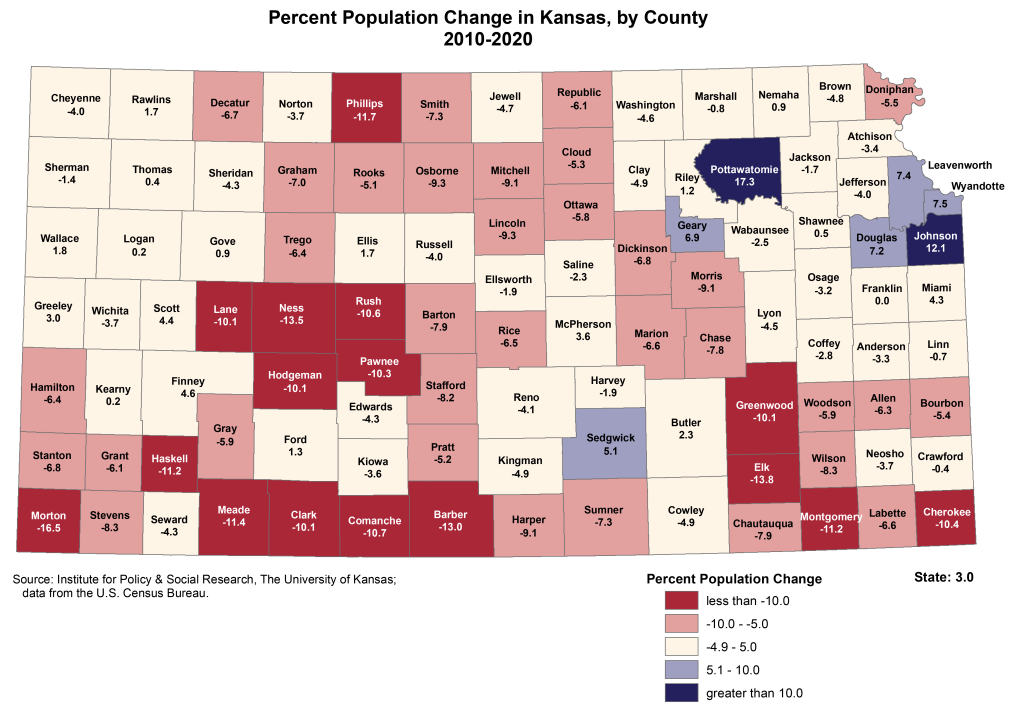
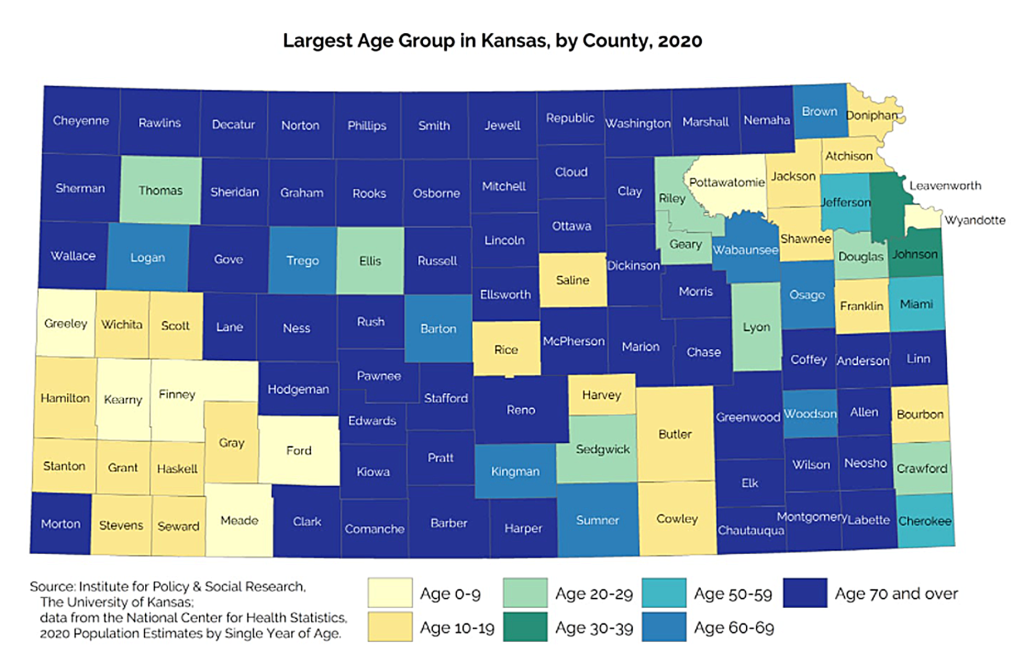
Our population is growing slowly, mostly in cities, and older, as depicted below. WSU CEDBR projects by 2064 a 33% decline in rural population, a 6.5% decline in micropolitan areas and that one quarter of Kansas residents will be over age 65. Older and rural populations tend to be less healthy and require additional care.
At the same time, over the past 20 years, the Kansas population has grown more diverse, a trend expected to continue. A 52.5% increase in minority populations (any group other than non-Hispanic White) generated the only population growth in Kansas this century.
That trend makes it critically important for Kansas to address longstanding racial and ethnic disparities in health, poverty rates and educational attainment. Training and hiring culturally competent health care workers will become increasingly important to addressing health inequities and building a health care system to meet future needs.
COVID-19 worsened an already inadequate supply of providers
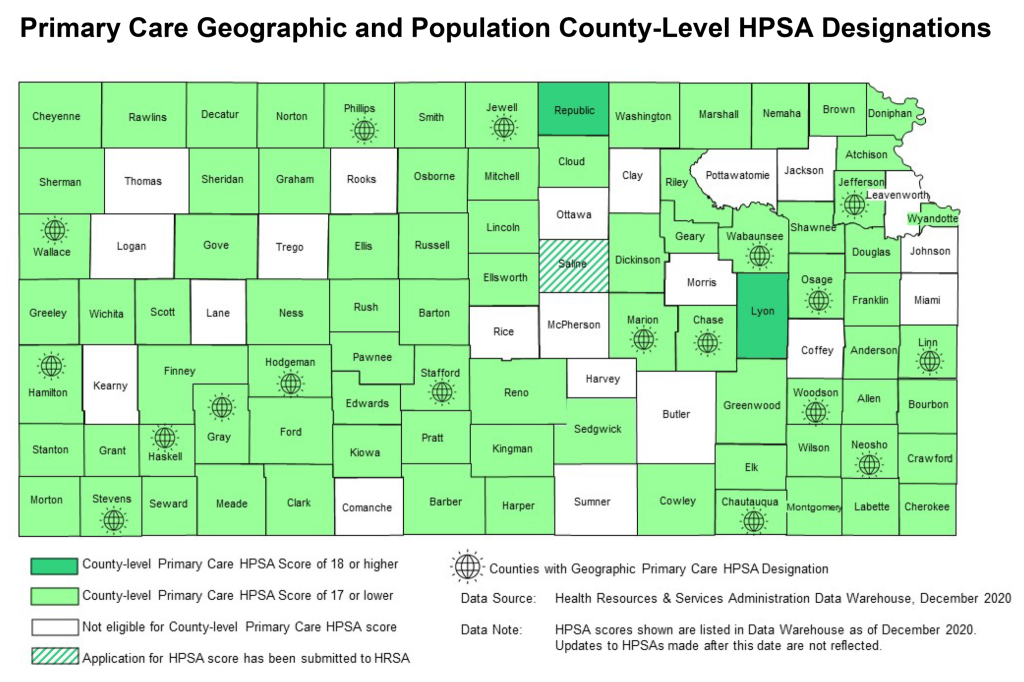
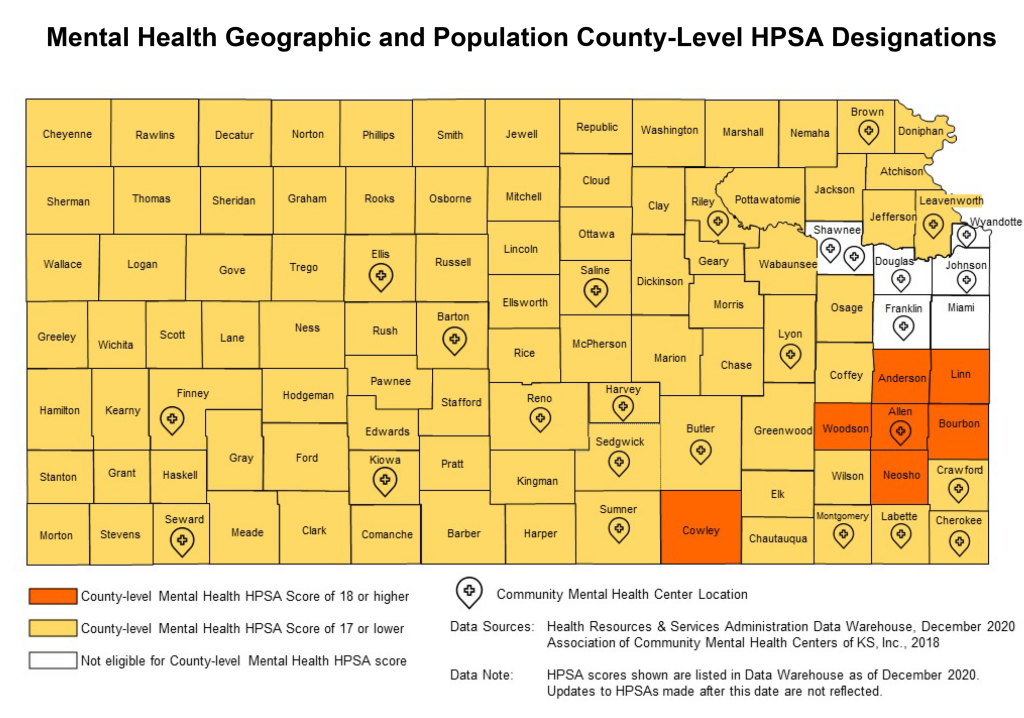
Before COVID-19, many Kansas counties already had an inadequate supply of health professionals. As the below Kansas Department of Health and Environment figures depict, the majority are considered health professional shortage areas (HPSAs) for both primary and mental health care — lacking the health professionals necessary to meet their population’s health care needs.
COVID-19 exacerbated that existing workforce challenge. In a 2021 KFF report, 3 in 10 health care workers said due to the pandemic they have considered leaving health care. Earlier this year, McKinsey and Company reported 32% of RNs surveyed in November 2021 said they may leave in the next year.
Provider retirements will create additional pressure – a Kansas Health Institute brief illustrates that in 2020, nearly 4 in 10 (39.2%) of primary care providers in Kansas were over the age of 55, rising to nearly half in some regions (45.2% in southwest Kansas and 42.5% in southeast Kansas).
Kansas lags national insurance rates, reducing competitiveness for health care professionals
Uninsured patients and resulting uncompensated care complicate financial sustainability for health systems, impacting daily operations and long-term viability of health care — especially in rural communities and communities of color.
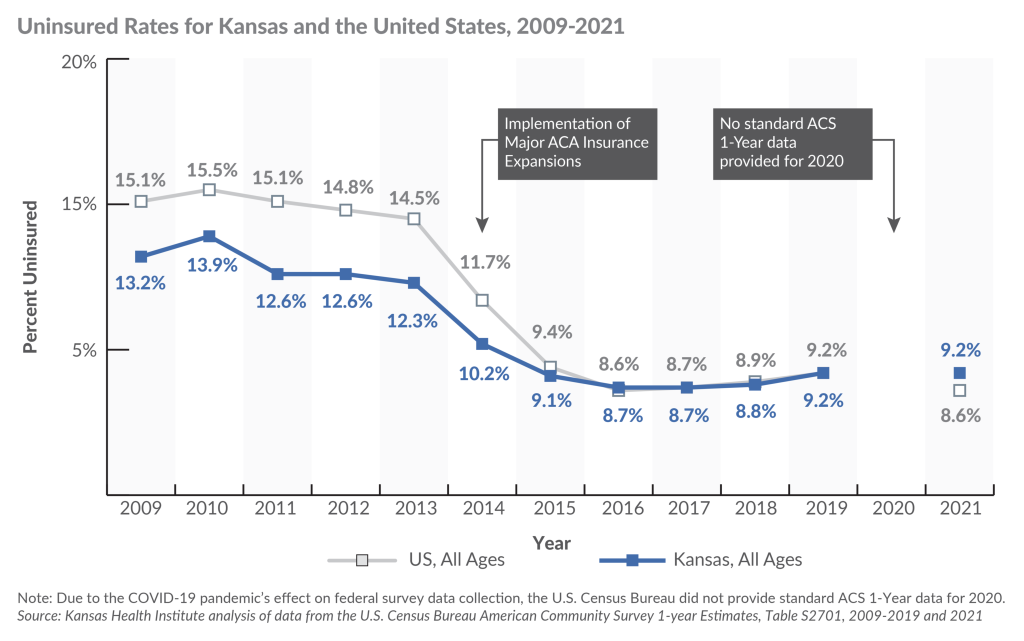
Kansas is one of 12 states that have not expanded Medicaid, evidenced in our stagnant uninsurance rate. According to KHI, as the national uninsurance rate declined to 8.6% in 2021, Kansas’ rate remained at 9.2%. This was the first time in decades our uninsurance rate exceeded the national average. The difference in 2021 primarily reflects a higher uninsured rate in Kansas versus the U.S. among working-age adults.
Historically, uninsured rates in rural counties are among the highest in Kansas. There are also significant disparities among Kansas residents by race and ethnicity. Those identifying as Hispanic or Black are more likely to be uninsured in Kansas than the United States. In Kansas, uninsurance rates were 20.3% for Hispanic residents and 14.1% for Black or African American, versus 17.7% and 9.6% U.S. averages, respectively.
Before implementation of the Affordable Care Act, Kansas boasted a better uninsurance rate than the national average but now lags.
Beyond higher-than-national-average uninsured rates, the failure to expand Medicaid negatively affects hospital finances and results in more uncompensated care. In fact, 44.3% of uncompensated care in critical access hospitals in Kansas could be eliminated by expanding Medicaid. Because Kansas has not expanded Medicaid, we have more financially vulnerable hospitals than any other state.
The high uninsured rate and financial instability make us less competitive in recruiting providers versus surrounding states that have all expanded Medicaid.
In part two of this series, we’ll move beyond the challenges and explore how Kansans are collaborating to develop innovative solutions. To learn more, visit https://communityconversationsks.com.
Back to All News