This guest blog post was authored by Brenda Bandy, IBCLC, and Jennie Toland, BSN, RN, CLC, Co-Executive Directors of the Kansas Breastfeeding Coalition.
“[…] exclusive breastfeeding goes a long way toward canceling out the health difference between being born into poverty and being born into affluence…It is almost as if breastfeeding takes the infant out of poverty for those first few months in order to give the child a fairer start in life […]”
– James P. Grant, former UNICEF executive director
We are thrilled to report the state of breastfeeding in Kansas is strong! According to data from the Centers for Disease Control and Prevention (CDC) released on August 1, Kansas exceeds the national rates of breastfeeding in all measures. Kansas ranks 14th in the nation in the percent of infants exclusively breastfeeding at 6 months of age for babies born in 2019. This is up from 27th place only five years ago.
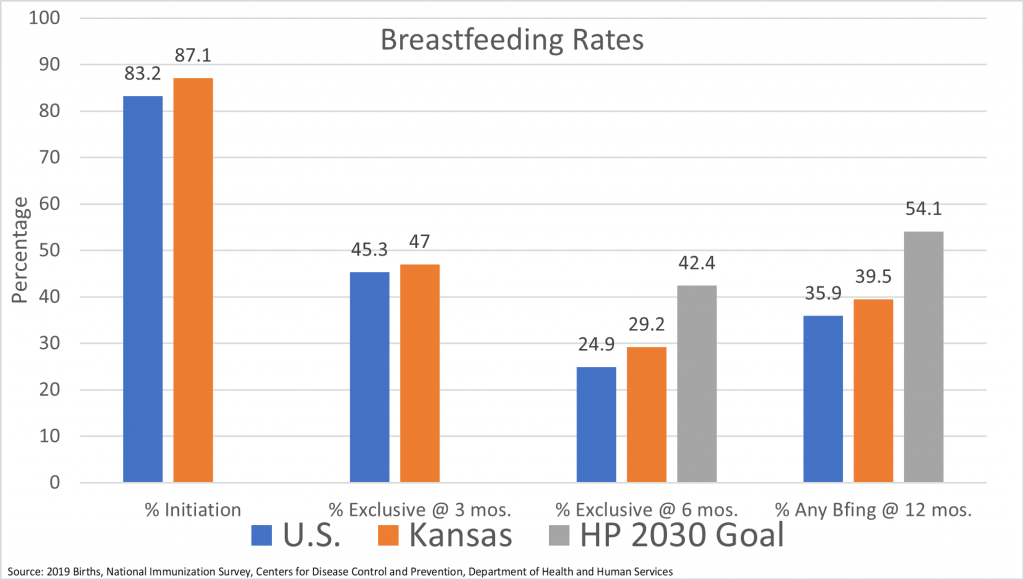
The data show nearly 90% of families in Kansas choose to breastfeed. However, the choice to breastfeed is negatively influenced by lack of support in the workplace, lack of access to clinical and peer lactation support, and often lack of family support. Without the right support, the choice to breastfeed isn’t a choice at all.

Consider this map above of breastfeeding initiation rates by county. The counties in pink exceed the state average in breastfeeding initiation rates. The counties in white have the lowest rates of breastfeeding initiation. Social determinants of health can greatly impact breastfeeding rates. We must carefully consider what factors are making it difficult for families to be able to choose to breastfeed.
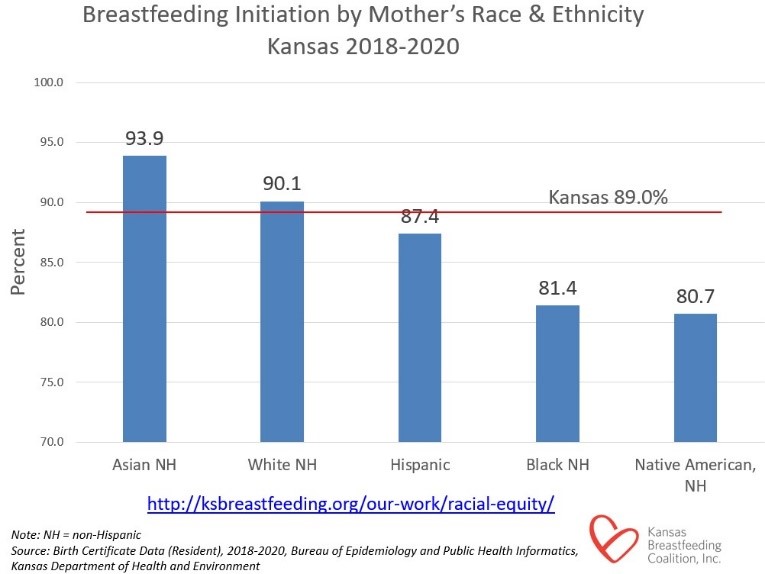
The graph above illustrates the gaps in breastfeeding rates. These disparities result from structural barriers and historical trauma that make it more difficult for Black, Indigenous and Latina mothers to engage in a traditional practice that has sustained their cultures over generations. While Black and Indigenous families do breastfeed, they do so despite bias and inequities.
The KBC has taken the following action to address racial disparities in breastfeeding rates with support from our partners at the Kansas Department of Health and Environment (KDHE) and the United Methodist Health Ministry Fund (Health Fund):
- Compiled research and resources on our Equity pages for racial & ethnic, geographical and LGTBQIA+ equity
- Compiled resource pages for Black, Indigenous, and Latinx families
- Supported Chocolate Milk Café facilitators in Kansas City, Topeka and Wichita
- Launched a scholarship program to help diversify the lactation workforce
- Supported the formation of Black, Indigenous and Latinx breastfeeding coalitions
How can we make impactful and sustainable improvements to breastfeeding? The answer lies within the community. It is our responsibility to support communities and ensure they have needed resources. While we celebrate increased breastfeeding rates in Kansas, a “rising tide” of breastfeeding support is not enough when some families in Kansas are not even in a boat.
The American Academy of Pediatrics’ (AAP) new Position Statement: Breastfeeding and the Use of Human Milk highlights the importance of supportive policies and systems. The AAP statement recommends “Policies that protect breastfeeding, including universal paid maternity leave, the right of a woman to breastfeed in public, insurance coverage for lactation support and breast pumps, on-site child care; universal workplace break time with a clean, private location for expressing milk, the right to feed expressed milk, and the right to breastfeed in child care centers and lactation rooms in schools are all essential to supporting families in sustaining breastfeeding.”
The KBC and our partners, including the Health Fund and KDHE, are working on improving policies, systems and environments to be more supportive of breastfeeding families.
A recent policy “win” for families in Kansas was the extension of Medicaid postpartum coverage for mothers from a mere 60 days to a full year. This extension of access to coverage will increase access to breastfeeding support in addition to essential physical and mental health services during the first year after giving birth.
Many hospitals across Kansas have contributed to the rising breastfeeding rates in Kansas. Thanks to the Health Fund’s investment in High 5 for Mom & Baby, Kansas ranks 13th in the nation for maternity care practices as measured by the CDC Maternity Practices in Infant Nutrition and Care survey.
If you are curious what breastfeeding support looks like in your county, visit the KBC’s Breastfeeding Support by Kansas County. This document allows you to easily see not only breastfeeding rates but also peer, clinical, and systems-level support for breastfeeding.
We invite you to join the Kansas Breastfeeding Coalition to build on this momentum and continue to improve policies, systems and environments to support Kansas families to breastfeed.
Please consider taking the following actions to support breastfeeding in your community.
ACTION IDEAS
INDIVIDUALS CAN:
- Smile at a parent breastfeeding in public.
- Join or form a local breastfeeding coalition.
- Find breastfeeding help using the KBC’s Local Breastfeeding Resource Directory.
- Choose High 5 for Mom & Baby recognized or Baby-Friendly designated hospitals.
- Choose designated Breastfeeding Friendly Child Care Providers.
HEALTHCARE PROVIDERS CAN:
- Attend breastfeeding education opportunities.
- Counsel parents on breastfeeding during prenatal visits and encourage families to attend breastfeeding education opportunities.
- Encourage physician practices to adopt breastfeeding supportive practices.
BUSINESSES CAN:
- Participate in the Breastfeeding Welcome Here campaign.
- Support breastfeeding employees in the workplace.
- Participate in local and state breastfeeding coalitions.
- Ensure employee insurance covers double electric breast pumps.
- Provide paid family leave.
HOSPITALS CAN:
- Become recognized as a High 5 for Mom & Baby hospital by implementing at least five evidence-based maternity care practices.
- Become designated a Baby-Friendly Hospital by implementing the Ten Steps to Successful Breastfeeding.
- Participate in the KBC’s Hospital Section.
- Support staff to learn more about breastfeeding.
STATE AND LOCAL GOVERNMENT CAN:
- Help hospitals connect parents to community breastfeeding resources once they leave the hospital.
- Support and participate in local breastfeeding coalitions.
- Support paid family leave.
- Support KanCare coverage of lactation and doula services.
About the series
This is the second post in a series on breastfeeding in Kansas. The full blog series includes: