Welcome to the Pioneers in Health podcast. In this podcast, we share inspiring stories of pioneering leaders from our nation and from your backyard who are working to improve health.
In episode 24, we interview Becca Graves, executive director at Perigee Fund. The Perigee Fund is a philanthropy that focuses on increasing support for families impacted by trauma. It invests in systems change to ensure that during pregnancy and early childhood, more families receive healing programs, services and resources that protect and nurture their unfolding relationships.
In this episode, Becca discusses her economic mindset and a twist of fate that led to her working in philanthropy.
She discusses how in a previous role she was part of many conversations where people discussed the long-term impact of childhood trauma on adults or how to support high school students who had experienced early trauma.
“I was always in the room thinking, why are we not doing something earlier?” Becca said.
“Mental health begins before birth, and the well-being of parents as they expect a child is incredibly important.”
– Becca Graves
Becca discusses the importance of this and how it’s critical to address mental health during pregnancy, as it’s not only important for the parents, but it’s also where mental health for a child begins.
“Mental health begins before birth, and the well-being of parents as they expect a child is incredibly important,” she said. “Maternal mental health complications during pregnancy and postpartum are incredibly common. Maternal depression is the one of the original ACEs. And, largely, maternal mental health complications are preventable and treatable.”
ACEs refers to Adverse Childhood Experience score, which is derived from a questionnaire that measures exposure to different types of adverse childhood experiences, such as abuse, neglect or household dysfunction.
“Addressing the well-being of children absolutely starts with their caregivers,” Becca said.
Perinatal mental health specialists are few and far between, she said, so she said they’ve invested in perinatal psychiatry around the country for physicians.
She also discussed Perigee’s efforts to affect policies and system change, which often centers on efforts to treat the baby and caregiver as a family unit instead of as individuals. At this stage of life, the relationship between the two is critically important.
“They should receive care that is connected,” she said. “There is a phrase in the infant mental health world that there’s no such thing as a baby on its own. It’s always a baby and a caregiver together. So, a lot of the policy innovation can be very, very specific to changing practice to serve the family as a unit.”
In this episode, she also discusses:
Her journey to working at the Perigee Fund
Perigee’s approach to mental health
How addressing the well-being of children starts with addressing the caregivers’ well-being; she mentions the Attachment and Biobehavioral Catch-up home-visiting program, a model the Health Fund supported to determine its efficacy in Kansas
How health insurance, including the public health insurance program Medicaid, is critical for helping mothers and babies
The importance of nurturing the bond between parents and their child
The Health Fund commissioned a report by KU School of Nursing, who worked in collaboration with the Kansas Center for Rural Health, to conduct research on access to maternity care in Kansas. The report was released May 8, 2025. This story below announcing the reportoriginally appeared on KU Medical Center’s website.
Report describes the state’s maternity care desert and provides detailed information on the critical resources needed to ensure healthy mothers and babies
May 8, 2025 | Kristi Birch, KU Medical Center
Access to quality care during pregnancy and after birth, often difficult to access in rural areas, is critical to the health of newborn babies and their mothers.
The growing maternal-care desert in Kansas is causing more women in the state to drive long distances for care and 59% do not have local access to inpatient maternity services, according to a report released today by the University of Kansas School of Nursing.
Over the last 10 years, many rural hospitals across the country have closed or have stopped offering maternity care services altogether. This includes in Kansas, which is second only to Texas in terms of the number of counties considered rural. Rural hospitals are at an increased risk of closure due to declining occupancy rates, high fixed costs and market pressures.
“Kansas legislators, health care systems, foundations, professional organizations and educational institutions are all working hard to address the concerns of access to care and the health care workforce,” said Karen Weis, Ph.D., FAAN, dean of KU School of Nursing-Salina and lead author of the report. “Sound data is needed to support these efforts. The Access to Maternal Care in Kansas report is a first step in gathering that data in one central source.”
Access to quality perinatal care, which includes care during pregnancy and after the birth, is critical to the health of newborn babies and their mothers. Closures of hospitals and cessation of maternity services are correlated with more babies being born early, more infants admitted to neonatal intensive care units and more women dying during pregnancy or in childbirth.
The report outlines, by county and ZIP code when possible, the numbers of women of reproductive age in the area, the facilities offering prenatal care or inpatient maternity care; the availability of referral and high-risk services; and the providers accepting patients and offering prenatal or full perinatal services, nursing, anesthesia, behavioral health, lactation, and doula support services. It also provides the distances to facilities with delivery capabilities.
Karen Weis, Ph.D., FAAN, dean of KU School of Nursing-Salina
Key findings in the report, which is based on data from 2022-2024, include:
An increasing number of Kansans travel up to 60 miles for low-risk prenatal and postpartum and labor and delivery care, particularly in the central and southwest parts of the state.
Fifty-nine percent of Kansans do not have local access to inpatient maternity care.
The availability of services for women with high-risk pregnancies is extremely limited. Close to 30% of ZIP codes in Kansas are more than 100 miles away from tertiary, high-risk services.
Forty-two counties in Kansas are without any documented anesthesia providers, and most of those are on the western side of the state.
The report also found that the counties with the highest birth rates are the ones losing access to maternity care services. And rural counties had higher birth rates than urban ones: 67 versus 61 live births per 1,000 women of reproductive age.
“To me, the biggest surprise in the report are the two counties in western Kansas with the highest birth rates,” said Weis. Neither of these counties, Wallace and Grant, have a health care system offering maternity care. The distance to inpatient maternity care for those residing in each county is approximately 50 miles and 24 miles, respectively.
The report also provides information clarifying the unrecognized costs of providing maternal health care, which requires the presence of multidisciplinary teams of providers and nurses 24 hours a day, 7 days a week, 365 days a year. The vast majority of rural hospitals are reimbursed through a Medicare-reimbursement model, which does not cover the high cost of providing maternity care.
“These data paint a stark picture of the current landscape of access to maternal health. The data also emphasize the critical importance of addressing this challenge before it gets worse, as well as recognizing that the location of services is one piece of the puzzle,” said David Jordan, MPA, president and chief executive officer of United Methodist Health Ministry Fund, which is based in Hutchinson, Kansas. “We need to figure out solutions to complete the puzzle in order to provide women, children and families across the state with better access to the services they need to thrive.”
Earlier this month, Kansas was awarded a $17-million, 10-year grant to participate in the Centers for Medicare & Medicaid Services’ Transforming Maternal Health (TMaH) Model.
This model has the potential to revolutionize the way maternal health care is provided in Kansas — a necessary action at a time when more than 45% of Kansas counties qualify as maternal health care deserts. Many women must travel more than 30 minutes — and sometimes 60 minutes — to reach their nearest birthing hospital.
We applaud Gov. Laura Kelly, the Kansas Department of Health and Environment and the state Medicaid agency for their leadership and for successfully securing this substantial grant that will prioritize the health and wellness of Kansas mothers and families.
“It’s critical we find ways to expand access to maternal health care in Kansas,” said David Jordan, Health Fund president. “Mothers across the state — and especially in our rural communities where services are disappearing — need and deserve this. The TMaH model will provide the funding and support necessary to make substantial steps forward in addressing this issue so that Kansas can create sustainable solutions to improve the lives of mothers, babies and families.”
The TMaH model focuses on improving maternal health care for people enrolled in Medicaid and the Children’s Health Insurance Program (CHIP). The goal is to reduce disparities in access and treatment, improve birth outcomes and experiences for mothers and their newborns, and reduce overall program expenditures.
1. Access to care, infrastructure and workforce capacity This includes addressing gaps in maternal care by improving access to valuable resources like midwives, doulas and community health workers. These care team members can reduce the number of c-sections for low-risk pregnancies, shorten labor time, lower the use of pain medication during birth and lower the rates of postpartum anxiety and depression.
2. Quality improvement and safety This includes implementing quality initiatives and protocols to make childbirth safer while improving the mother and baby’s overall experience. When implemented together consistently, these protocols have been shown to improve health outcomes.
3. Whole-person care and delivery This includes working with mothers to develop a unique birth plan that will support their physical, social and mental health needs. This may even include remote monitoring of conditions like hypertension and diabetes to reduce the burden of traveling to and from a doctor’s office. It could also include connecting a mother with community organizations or a community health worker.
As part of the participation in the model, Kansas will also be required to develop and implement a health equity plan that addresses disparities among underserved populations.
These are all significant steps in the right direction, as we work to find solutions that will improve access to care for our state’s mothers.
“This was a monumental win for maternal health care in our state,” Jordan said. “Thanks to this funding, the state will be able to expand its workforce and improve the health of mothers and children. We look forward to seeing the impact this will make throughout Kansas.”
JUST ADDED! Webinar: “Access to Maternity Care in Kansas” 11-12 p.m. Thursday, June 12, 2025
The growing maternal-care desert in Kansas is causing more women in the state to drive long distances for care, with 59% not having any local access to inpatient maternity services.
The KU School of Nursing recently released a report detailing the availability of maternity care across Kansas. The report, “Access to Maternity Care in Kansas,” was produced in collaboration with the Kansas Center for Rural Health with funding from the United Methodist Health Ministry Fund.
Over the last 10 years, many rural hospitals across the country have closed or have stopped offering maternity care services altogether. This includes in Kansas, which is second only to Texas in terms of the number of counties considered rural. Rural hospitals are at an increased risk of closure due to declining occupancy rates, high fixed costs and market pressures.
Access to quality perinatal care, which includes care during pregnancy and after the birth, is critical to the health of newborn babies and their mothers. Closures of hospitals and cessation of maternity services are correlated with more babies being born early, more infants admitted to neonatal intensive care units and more women dying during pregnancy or in childbirth.
The report outlines, by county and ZIP code when possible, the numbers of women of reproductive age in the area, the facilities offering prenatal care or inpatient maternity care; the availability of referral and high-risk services; and the providers accepting patients and offering prenatal or full perinatal services, nursing, anesthesia, behavioral health, lactation, and doula support services. It also provides the distances to facilities with delivery capabilities.
Learn more about the findings from this report during a special webinar from 11-12 p.m. Thursday, June 12, via Zoom. Speakers will include the report’s lead author, Karen Weis, Ph.D., FAAN, dean of KU School ofNursing-Salina, followed by a panel discussion with maternal and rural health experts.
The Kansas Department for Children and Families’ child care subsidy program is one of the most important tools used to address child care affordability in the state.
However, just 12% of eligible families are participating in the program. Family participation in the program is tied to provider availability and provider participation in the program.
To gain insight as to why providers participate or not, the United Methodist Health Ministry Fund partnered with Kansas State University to survey Kansas child care providers to better understand their perception and experience with DCF’s child care subsidy program.
Join this webinar to discuss key findings from this important survey, “Child Care Providers: Perception of Child Care Subsidies in Kansas.”
Leveraging the CCBHC Model to Enhance Childhood Mental Health 1-2 p.m. Thursday, Nov. 14, 2024
The years from birth to age five are critical for a child’s development, with rapid brain growth and increased neural connections laying the groundwork for cognitive, emotional and social skills that last into adulthood.
In Kansas, there has been progress in recognizing the importance of infant and early childhood mental health and expanding access to services for young children and their families.
However, challenges remain.
The Certified Community Behavioral Health Clinic (CCBHC) model presents a framework to address these gaps — emphasizing comprehensive, person-centered care through strategic partnerships, workforce development and targeted interventions.
Kansas has an opportunity to strengthen its system for delivering infant and early childhood mental health services, leveraging the model’s services and payment structure to ensure that all children and families can benefit from timely and effective support.
The Health Fund recently partnered with the Kansas Health Institute to research this opportunity. Learn more about this during our upcoming webinar, “Leveraging the CCBHC Model to Enhance Childhood Mental Health.”
Social-emotional development in young children is a critical factor related to later-life outcomes, such as school success, social interactions and mental health.
A growing body of research demonstrates that investing in science-based, short-term early interventions pays off over both the short and long term, delivering lasting results that not only change lives for the better but also produce substantial returns on that investment.
The Attachment and Biobehavioral Catch-up (ABC) program is an evidence-based, home visiting intervention for caregivers of infants and toddlers who have experienced early adversity. It is designed to buffer the harmful effects of toxic stress and help support normal early childhood development.
To explore the effectiveness of ABC with Kansas families, the KU School of Social Welfare (supported by multiple Kansas philanthropies, including the Health Fund) worked with several early childhood and mental health organizations across the state to research this program.
Now, seven years later, the Kansas ABC Early Childhood Initiative has concluded.
This webinar discussed the promising results from Phase II of this project, which continued researching the program’s effectiveness with infants and expanded to include toddlers with their caregivers.
The registration form is now closed – thank you for your interest. Please contact David Jordan david@healthfund.org for waiting list or future events.
Stay tuned, as we will be adding additional webinars to this series! Subscribe to our emails or follow us on social media to find out the latest topics added.
In 2017, the United Methodist Health Ministry Fund Board of Directors voted to honor the organization’s founding president with the establishment of the Kim Moore Award for Visionary Leadership.
Each year, the Fund solicits nominations in a chosen strategic field of work and honors one individual whose leadership has had a positive effect on the health of a specific group of persons.
For 2024, the Health Fund is inviting nominations for a leader who has previously or is currently serving in the strategic area of Thriving Children.
The winner of the award will be honored at a ceremony in May 2025. The individual will receive a cash award of $500, and if associated with an organization, that agency will receive an additional $2,000 to use as it deems.
Please direct any questions about this award to Katie Schoenhoff, Vice President of Programs.
To nominate a candidate, please complete the online form below or include the same information in an email or letter to Katie Schoenhoff (katie@healthfund.org / United Methodist Health Ministry Fund, PO Box 1384, Hutchinson, KS 67504-1384).
Nominations need to be received in the Health Fund office by November 15. If you previously nominated an individual who was not selected, you are welcome to renominate that person for the 2024 award. This award is open to all Kansans, and no affiliation with the Health Fund is required.
In 2023, the United Methodist Health Ministry Fund awarded 117 grants, convened 14 public meetings, conducted three training series and secured $4 million in federal grant money for Kansas.
And that’s not all.
We continued to work closely with our existing partners and forged new relationships, as well, that will help us advance our goal of improving the health of all Kansans.
In our 2023 Year in Review report, which we just released, you can learn in greater detail about these efforts as we kicked off the first year of our new strategic plan.
Partnered with the Kansas Hospital Association to transition two traditional hospitals that were at risk of closure into Rural Emergency Hospitals.
THRIVING CHILDREN
Worked with partners to improve early childhood policies and services. We also launched research on the child care assistance program and family economic security issues, including child care.
Served on the Early Childhood Transition Task force. Health Fund President David Jordan was nominated by Governor Kelly to serve on this important task force to help recommend how the state can improve its early childhood services.
Helped increase access to early childhood mental health services by funding Parent Child Interaction Therapy training in several areas across the state.
Partnered with breastfeeding coalitions and health leaders to make significant gains in helping mothers initiate and maintain breastfeeding. Our funding also helped form coalitions led by women of color to support their communities in breastfeeding; it also increased access to lactation support services by helping certify more than 50 consultants and counselors.
Helped address food insecurity in Salina by providing grant funding for a three-month Summer Food Service Program. Our funding helped to purchase necessary equipment, including shelving and freezers, and signage for an onsite grab-and-go distribution point.
Reignited the annual Healthy Congregations Retreat for the first time since the pandemic in 2020.
Our impact in 2023 was significant, and our efforts continue. We look forward to furthering our mission in 2024 to help create a healthier Kansas.
The relationships that infants and toddlers form with their caregivers are foundational. Through strong attachment and nurturance, children are better prepared for school and to hit developmental milestones on time.
The second phase of the pilot is underway and focuses on creating healthier futures for toddlers. Our evaluation will measure executive functioning and child well-being, which are both related to school readiness.
“Investing early is an opportunity to help have a profound impact on the health and economic well-being of children and families,” said David Jordan, Health Fund president. “For every $1 invested you see a $7 return. Ultimately, we all share the goal of having healthier kids and families. ABC helps us get there for some of the most vulnerable Kansans. The results are promising, and the future is bright.”
This guest blog post was authored by Joyea Marshall-Crowley, CBS, Wichita Black Breastfeeding Coalition.
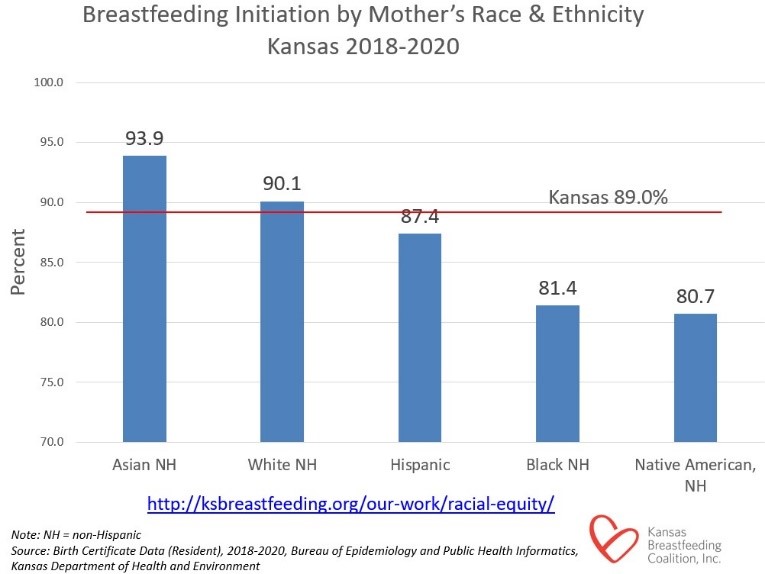
In the Wichita area, we have heard from Black and brown mothers that they are not even being asked about breastfeeding as an initial feeding choice, and that their healthcare providers assume they are formula-feeding their babies. This makes it difficult for Black and brown mothers to obtain breastfeeding resources, support, or information during pregnancy and upon delivery. It is imperative to have these supports for a woman’s breastfeeding journey, and it should be accessible to all mothers no matter their decision to breastfeed or not.
The need for the Wichita Black Breastfeeding Coalition is clear.
Who is the Wichita Black Breastfeeding Coalition?
The Wichita Black Breastfeeding Coalition (WBBC) was formed in October 2020 under the non-profit organization Kansas Breastfeeding Coalition. The foundational vision for this local breastfeeding coalition is to help increase breastfeeding rates in the Black and brown communities of the Wichita Metropolitan Area.
The coalition currently houses six members. The outstanding members of the WBBC hold many titles, such as Certified Breastfeeding Specialist (currently on track to obtain their IBCLC), Certified Trained Doulas, Registered Nurse, Chocolate Milk Certified Trainer, Chiropractor, and Midwife, to name a few.
All WBBC members share the same passion for helping women of color gain the support, resources, and tools needed to reach their breastfeeding goals. We want mothers of color to have a safe space just for them to receive the breastfeeding support they need—and that is what they will get from the Wichita Black Breastfeeding Coalition.
“I Breastfed; This is My Legacy”
Representation of Black women is so important when it comes to normalizing breastfeeding. This group is underrepresented, and there is already a stigma in the Black and brown community that breastfeeding is a “white” thing. When they see pictures and videos of breastfeeding mothers that heavily display white mothers as the focus it just reinforces the same message as the stigma and creates barriers.
To dispel this myth, the Wichita Black Breastfeeding Coalition created a project called “Latched Legacy.” This project highlights and normalizes that Black women do indeed breastfeed. The campaign video shows Black mothers confidently sharing the statement “I Breastfed; This is My Legacy” while capturing them with their children and partners. The project’s goal is not only to increase breastfeeding initiation rates in the Wichita Metro Area but also to increase media representation for Black mothers regarding breastfeeding.
“Latched Legacy” campaign video
In conjunction with representation, this project has also allowed us to provide breastfeeding kits for pregnant and breastfeeding mothers of color. These kits include supplies and information to encourage them to initiate breastfeeding as their first choice upon delivery. As a result, we have a success rate of 95% of mothers who have received a kit while pregnant initiating breastfeeding as their first choice of feeding after delivery.
Breastfeeding is for mothers of all backgrounds. We are changing the Black breastfeeding narrative one family at a time in the Wichita area. Every Kansas family should receive the resources and support they need to reach their breastfeeding goals. You can support new or expecting parents in your area by referring them to a local breastfeeding coalition or to an organization that provides breastfeeding resources.
About the series
This is the final post in a series on breastfeeding in Kansas. Prior posts include:
This guest blog post was authored by Heather Peterson RDN, LD, CLC, Reno County WIC Coordinator.
Every day, I look forward to going to work in WIC: we truly are the Happy, Healthy Baby People!
WIC is a supplemental food program that serves pregnant, breastfeeding, and postpartum women, infants, and children to age 5. Nearly half of all babies born in the United States are eligible for the WIC program. In Kansas, 40% of babies participate in WIC. This program has evolved over the past two decades from a formula handout to a reliable source of breastfeeding support. WIC promotes breastfeeding as the optimal way to nourish a newborn. All WIC staff encourage a pregnant woman’s decision to breastfeed.
A vast majority of women express a high desire to breastfeed their babies. Unfortunately, many of the women WIC serves return to work within two weeks of delivery. This can sabotage a woman’s desire to breastfeed. WIC offers several sources of support for breastfeeding moms.
The WIC food package for an exclusively breastfeeding woman is larger than any other food package and contains additional protein foods, including canned salmon or tuna. These fishes are higher in Omega-3 fatty acids that are important for infant brain development and overall health for the mom. Exclusively breastfeeding women enjoy a $47 per month fruit and vegetable benefit that allows them to purchase fresh fruits and vegetables. Women who are exclusively breastfeeding qualify for WIC foods until they are one year postpartum. Exclusively breastfed infants receive a large food package starting at 6 months of age to support their continued growth and development.
One major benefit of the program is that many local WIC agencies participate in the Breastfeeding Peer Counselor (BFPC) program. BFPCs are exactly what their name implies, women that have recently participated in the WIC program and breastfed their children. The BFPC usually communicates with women via text message, phone calls, and social media, and are even available to support breastfeeding parents outside of regular office hours.
Peer counselors will reach out to women during their pregnancy and offer reliable information about preparing to breastfeed, surrounding themselves with breastfeeding advocates, how to obtain a breast pump from their insurance, and what to expect the first days after delivery. Peer counselors can be a “social event director,” connecting pregnant and breastfeeding women in their community. Peer counselors will seek activities that are free of charge, such as playing at the splash pad, attending library time, gift-wrapping parties, and moms’ movie night out. One of our most popular events was a cooking class hosted by a local church. The foods were donated and each family took home a chicken noodle casserole they learned to prepare. This social time allows pregnant women to see how normal breastfeeding happens out and about whether the breastfeeding mom chooses to be discreet or open.
Photos from Breastfeeding Peer Counselorevents.
In the near future, families will have another trusted breastfeeding resource. Soon, each WIC agency will be required to have a Designated Breastfeeding Expert. This person handles more challenging breastfeeding issues. Breastfeeding is a learned skill. For some families, this comes easily and for others, there are more bumps in the road. Many physician’s offices will refer patients to WIC because they know there is reliable breastfeeding help available.
Sharing information about supports like WIC is something we can all do to support parents. It’s easy to determine WIC eligibility. Potential participants can find their local WIC office by visiting signupWIC.com and entering their ZIP code. To participate in the Kansas WIC program, families must reside in Kansas and meet income guidelines, which can be found at kdhe.ks.gov.
As a community, we can help families to meet their breastfeeding goals. Supporting paid maternity leave legislation, creating breastfeeding-friendly work environments, designating a private space for a woman to breastfeed if that is her preference, and learning about the amazing benefits of breastfeeding are all things we can do to create an environment that encourages breastfeeding success.
About the series
This is the fourth post in a series on breastfeeding in Kansas. Other posts include:
“I think it’s time for mommy milk!” said my 5-year-old to my 2-year-old as their 1-month-old baby brother began to fuss. “Mommy milk” has always been the term for breast milk in our house, coined by our eldest when her sister was born.
While celebrating National Breastfeeding Month, I remember my own breastfeeding experience. I was fortunate to successfully breastfeed all three of my children. I even had enough stored milk with my oldest two children that I was able to donate to a human milk bank.
My breastfeeding journey was relatively “painless” compared to others – if you don’t count the predicted engorgement, leaking, sore nipples, thrush for both me and my infant, and associated frustrations with finding appropriate times to pump while at work. (Thankfully, I had a very understanding employer.)
As a pediatrician and International Board Certified Lactation Consultant, I also have the privilege of being part of the breastfeeding/chestfeeding journey with many of my patients and their caregivers as they work to provide nutrition for their infants. Not all of their journeys were as “painless” as mine. One case in particular stands out – a mother who came to me with her 2-month-old infant. The case was referred to me due to the infant’s poor weight gain. I worked with the mother and child over the course of about 2 years. We tried different techniques to support weight gain including different ways to give expressed breast milk, different feeding routines, elimination diets for mom, creative ways to introduce solid foods, and so many other things. We involved specialists in different fields to help support the child and mother. Ultimately, the baby did well and was growing and thriving the last time that I saw her. Her mother worked tirelessly to provide the nutrition that she needed to ensure adequate growth, even though it was not the breastfeeding journey the mother would have imagined for herself.
Why breastfeed? The importance of human milk (in brief)
Physiological Benefits to the Infant
Human milk has been proven to be the optimal source of nutrition for infants.
There are multiple aspects in the dynamic properties of breast milk including antimicrobial, anti-inflammatory, and immunoregulatory agents which contribute to the developing immune system of the infant and help prevent infection.
Breastfeeding can reduce the risk of Sudden Infant Death Syndrome (SIDS), certain types of autoimmune disease (inflammatory bowel disease, diabetes mellitus, asthma, atopic dermatitis), leukemia, and obesity.
Physiological Benefits to the Mother
The act of breastfeeding can be beneficial to maternal health in helping mothers recover more quickly from childbirth, assisting with postpartum weight loss, reducing the risk of ovarian and breast cancer, reducing the risk of hypertension, and reducing risk of type 2 diabetes.
Intangible Benefits
Breastfeeding or chestfeeding facilitates maternal and infant bonding.
Breastfeeding can ultimately lead to a closer and more responsive infant/mother dyad.
It’s shown to reduce maternal stress and decrease cognitive and behavioral problems later in childhood.
What does the American Academy of Pediatrics say about breastfeeding and how do we promote and support breastfeeding mothers and their babies?
Exclusive breastfeeding for the first 6 months of life (consistent with guidelines provided by World Health Organization, American College of Obstetricians and Gynecologists, American Academy of Family Physicians, and Canadian Pediatric Society)
Continued breastfeeding along with appropriate complementary foods introduced at 6 months for as long as desired, 2+ years
Recognize that medical contraindications to breastfeeding are rare
Birth hospitals and centers should implement maternity care practices shown to improve breastfeeding initiation, duration, and exclusivity
National tracking of breastfeeding rates through age 2 years
Policies should be in place to protect breastfeeding
Universal paid maternity leave
Right to breastfeed in public
Insurance coverage for necessary items and care in breastfeeding
On-site child care in the workplace
Universal break time and adequate accommodations for human milk expression at work
Recognize that pediatricians (and all those caring for infants) play a critical role in breastfeeding success
Providing evidence-based information on feeding choices
Supporting early skin-to-skin contact and skilled lactation support while in the hospital
Using current resources to give guidance and minimize disruptions in breastfeeding when questions arise due to maternal medications, medical conditions, or vaccinations
Acquiring up-to-date information on the benefits of breastfeeding and how to provide breastfeeding care in the office and the community
Advocating for culturally sensitive and appropriate policies to promote breastfeeding
Assisting parents with preterm infants on establishing milk supply when infant is unable to feed at the breast and the use of pasteurized donor human milk
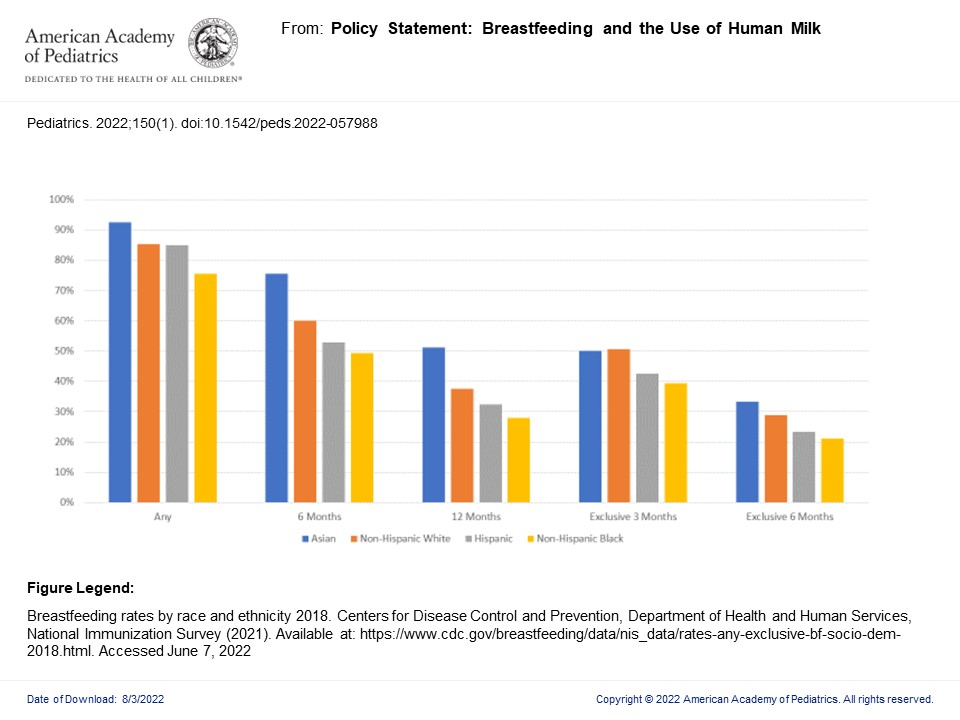
The graph above shows 2018 national breastfeeding rates for the infants in the breastfeeding dyad exclusively at 3 and 6 months of life, 6 and 12 months of life, and any breastfeeding at all throughout 0-12 months of life. Each age range is broken down into race and ethnicity at that stage. As evidenced above, we are making progress in supporting our lactating mothers and breastfeeding infants but there is always room for improvement. The education is ongoing as we strive to advocate for the breastfeeding dyad.
There are two excellent local upcoming opportunities for education as we welcome Dr. Joan Younger Meek to Grand Rounds at Wesley Medical Center in Wichita, KS, on September 15, and at the Kansas Chapter of the AAP Fall CME Meeting at Hyatt Regency Hotel in Wichita, KS, on September 16. Dr. Meek is the lead author of the new policy statement published July 2022 on “Breastfeeding and the Use of Human Milk” in the Journal of Pediatrics and a leading expert on breastfeeding and lactation. Please attend her presentations if you have the chance. In the meantime, Happy National Breastfeeding Month!
About the series
This is the third post in a series on breastfeeding in Kansas. Other posts include: